
Shantaquilette Carter-Williams was on the gymnasium treadmill when she first felt an odd flutter in her coronary heart. “I keep in mind stopping and considering, ‘That does not really feel proper,’” says the now 43-year-old Dallas resident. However she knew the significance of train—she walked or ran virtually every single day—so she acquired again to it and completed her exercise.
She adopted up with a physician who identified her with exercise-induced arrhythmia and advised her to watch out with rising her coronary heart price, says Carter-Williams, a retired accountant. She switched to totally different sorts of exercises. That was in 2012. Over the subsequent six years worrying signs resembling chest ache took her to the emergency room a dozen instances. Every time medical doctors there despatched her dwelling with no prognosis and no solution to stop it from occurring once more. In June 2018 lingering again ache, stomachache and nausea led Carter-Williams to assume she had the flu. She was working from dwelling and deliberate to go to mattress early, as an alternative of constructing one other inconclusive journey to the hospital. She was simply wrapping up a cellphone name when her college-aged daughter stepped into the room. Carter-Williams turned to talk, and a weird ache shot down the left aspect of her jaw and neck. “I might by no means felt something prefer it earlier than,” she says.
Her daughter drove her to the hospital. As they waited to be seen, Carter-Williams started to vomit. An intense stress, “like somebody stepping on my chest,” overwhelmed her. She was handed a tablet to position in her mouth. Then her coronary heart began to race. She remembers that hospital workers gave her an injection in her stomach and administered different medication. A brown-skinned physician got here into the room shortly after. He leaned over, held her hand and stated, “I do not wish to scare you, however you are having a coronary heart assault.”
After the specialist left, her personal heart specialist, who was a resident on the hospital, took over her care. She was discharged just a few days later with no medicine to stop one other incident—opposite to frequent medical suggestions. Because it seems, that is not an unusual state of affairs. “Sadly, guideline-based therapies aren’t uniformly utilized to all sufferers,” says Roxana Mehran, a heart specialist at Mount Sinai’s Icahn College of Drugs in New York Metropolis. “Ladies and underrepresented minorities are much less usually handled with guideline-directed medical and interventional remedies.”
9 months later, at age 40, Carter-Williams had a stroke.
As a Black lady, Carter-Williams was at excessive danger of getting a coronary heart assault. Regardless of that, she can be among the many sufferers most definitely to be ignored in screening checks or have signs dismissed as not heart-related. Outdated considering holds that overeating or a sedentary life-style are the primary danger components. However discrimination can be lethal: each inside the U.S. and world wide, individuals who expertise gender, race, socioeconomic or different discrimination are way more prone to endure and die from coronary heart illness.
Understanding of coronary heart illness has dramatically expanded over the previous half a century. Within the Forties coronary heart illness brought about round half the deaths within the U.S. The epidemic precipitated a flood of analysis that resulted in landmark, lifesaving discoveries. Researchers discovered, for instance, that inactivity, smoking, alcohol consumption, and diets wealthy in fatty meals or salt raised an individual’s danger of coronary heart illness. They found how circumstances resembling diabetes and excessive lipid ranges elevated the probabilities of coronary heart assault or stroke and designed medication to stave off these risks. And for individuals who wound up in emergency rooms regardless of these measures, surgical advances resembling balloon catheters, stents or synthetic valves made coronary heart assaults much less lethal.

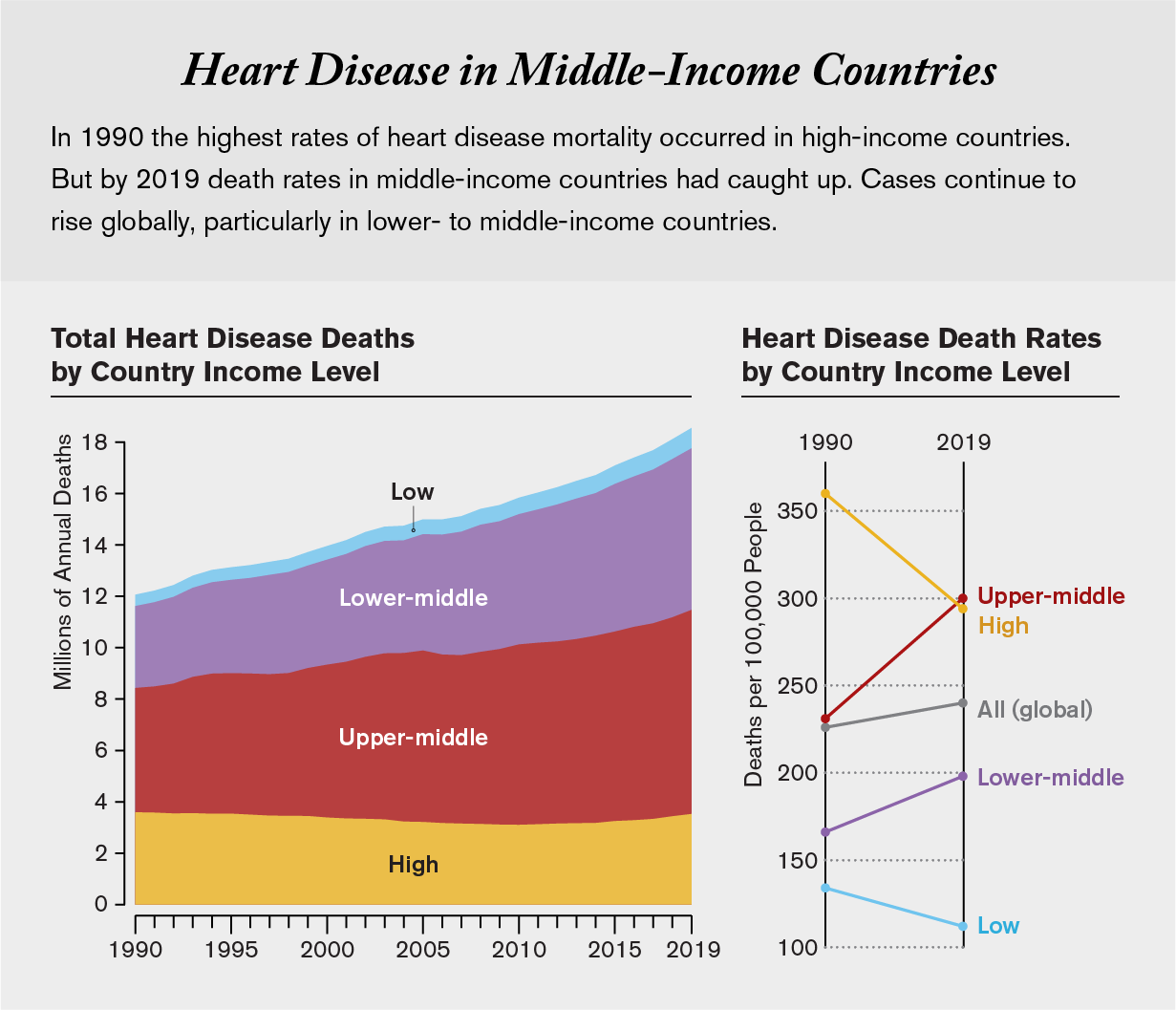
Over time deaths dropped—a minimum of in higher-income, majority communities in industrial nations. However as analysis on heart problems danger adopted a extra international strategy, coronary heart illness once more emerged because the number-one killer worldwide. These new research revealed that the identical danger components drove coronary heart assaults regardless of the place an individual lived or what their socioeconomic standing was. The distinction was that now about 80 % of coronary heart assault victims lived in lower- and middle-income international locations.
“For a lot too lengthy, we did not have high-quality research of heart problems that included folks” from lower- and middle- earnings international locations, says Amitava Banerjee, a heart specialist at College Faculty London. Throughout the U.S., analysis centered on higher-income communities. And in the remainder of the world, the main target was extra on the variations between Western and Jap international locations than on their similarities—one thing that, Banerjee says, stems from “a historical past of colonialism in drugs” that aimed to serve expats as an alternative of native communities.
Now researchers have centered on bridging these gaps. They’re exhibiting that, at each degree, advances in decreasing the burden of coronary heart illness are much less prone to attain or assist individuals who expertise discrimination. Lengthy-standing biases have resulted in medical remedies which might be much less accessible or, when accessible, much less helpful to traditionally marginalized communities. Not solely do these folks face limitations of entry, they’re additionally usually disproportionately burdened by danger components resembling air and water air pollution.
The biology of coronary heart illness is common. Checks, medication, and different interventions for decreasing coronary heart assault danger are the identical all over the place on the earth. Regardless of this shared basis, options addressing the issue had been principally developed inside a restricted, Western context. They fail to account for social circumstances that may make diagnostics, preventive drugs and coverings inaccessible to the remainder of the world. “We will not simply transport what we discover in high-income international locations and assume it may work in low-income international locations,” says Shivani Patel, a social epidemiologist at Emory College. “There are highly effective social influences that have to be included within the constellation of danger components.”
Ignored and Underrepresented
In 1947 the U.S. Public Well being Service (now the Nationwide Institutes of Well being) launched a examine that tracked each the well being and life habits of residents of the city of Framingham, Mass., after which checked out how these corresponded to coronary heart well being. Due to the Framingham Coronary heart Research—which continues at present—and others performed within the U.S. and Europe, clinicians now know exactly how coronary heart illness begins, worsens and kills. And so they know, to an important extent, learn how to cease it.
In 1990 William Kannel, a former director of the Framingham Research, gave a lecture by which he reported that the examine linked coronary heart illness to a “life-style typified by a defective eating regimen, sedentary dwelling, unrestrained weight achieve and cigarette smoking.” Subsequently, folks may enhance coronary heart well being by altering how they lived. Public well being campaigns world wide unfold the message. Within the U.S., the American Coronary heart Affiliation launched a marketing campaign, known as Life’s Easy 7, defining seven various things—resembling smoking, eating regimen and bodily exercise—that would lower cardiovascular danger.
Regardless of the title, these measures are something however easy. The recommendation to eat more healthy meals and be bodily lively is rooted in sturdy proof, but it surely doesn’t account for folks world wide whose lives look nothing like these of the principally white, principally well-off residents of a Boston suburb. “The present suggestions have fallen quick due to the shortage of deal with social determinants of well being and structural drivers” that affect an individual’s well being practices, says LaPrincess Brewer, a heart specialist on the Mayo Clinic in Minnesota. “Sadly, Life’s Easy 7 aren’t essentially delivered within the [appropriate] sociocultural context.”
Think about train. Even when possible, it’s not sufficient by itself to make sure a wholesome coronary heart. Carter-Williams knew train was necessary, notably as a result of her job got here with quite a lot of desk time. However a treadmill behavior wasn’t sufficient to stop her coronary heart assault. For others, simply strolling out the door is a troublesome ask. A scarcity of entry to protected areas for train, smog-filled air or cultural limitations to ladies strolling alone steadily hinder or stop bodily exercise. Patel factors to India for instance, the place persistent colorism drives ladies, notably adolescent women, to remain indoors (and thus be much less lively) to stop sun-darkened pores and skin.
Different instances recommending train is just absurd, says Andre Pascal Kengne, an internist and researcher on the South African Medical Analysis Council. In rural areas of South Africa, he factors out, folks prone to coronary heart illness usually work bodily demanding jobs, making deliberate train superfluous: “Consider a farmer who spends six to eight hours a day engaged on a farm,” he says. “In case you inform him at a seek the advice of to train, what do you count on to attain?”
Western dietary suggestions additionally fail to account for the way diets range by tradition. So-called heart-healthy meals described in public campaigns replicate a small subset of norms from industrial nations whereas excluding most culinary traditions world wide, together with within the U.S. Public campaigns goal for consciousness, however Brewer factors out that the issue for most individuals shouldn’t be a lack of information or information.
Translating consciousness right into a change in habits is stymied by many components: an absence of culturally related tips, monetary insecurity or an incapacity to entry reasonably priced, nutritious meals. “Whether or not it is their capacity to position meals on the desk or lack of retailers to buy wholesome meals,” Brewer says, group members are conscious they face these points. The issue, she says, is that they discover it powerful to behave on eating regimen or train suggestions given their monetary or social circumstances.
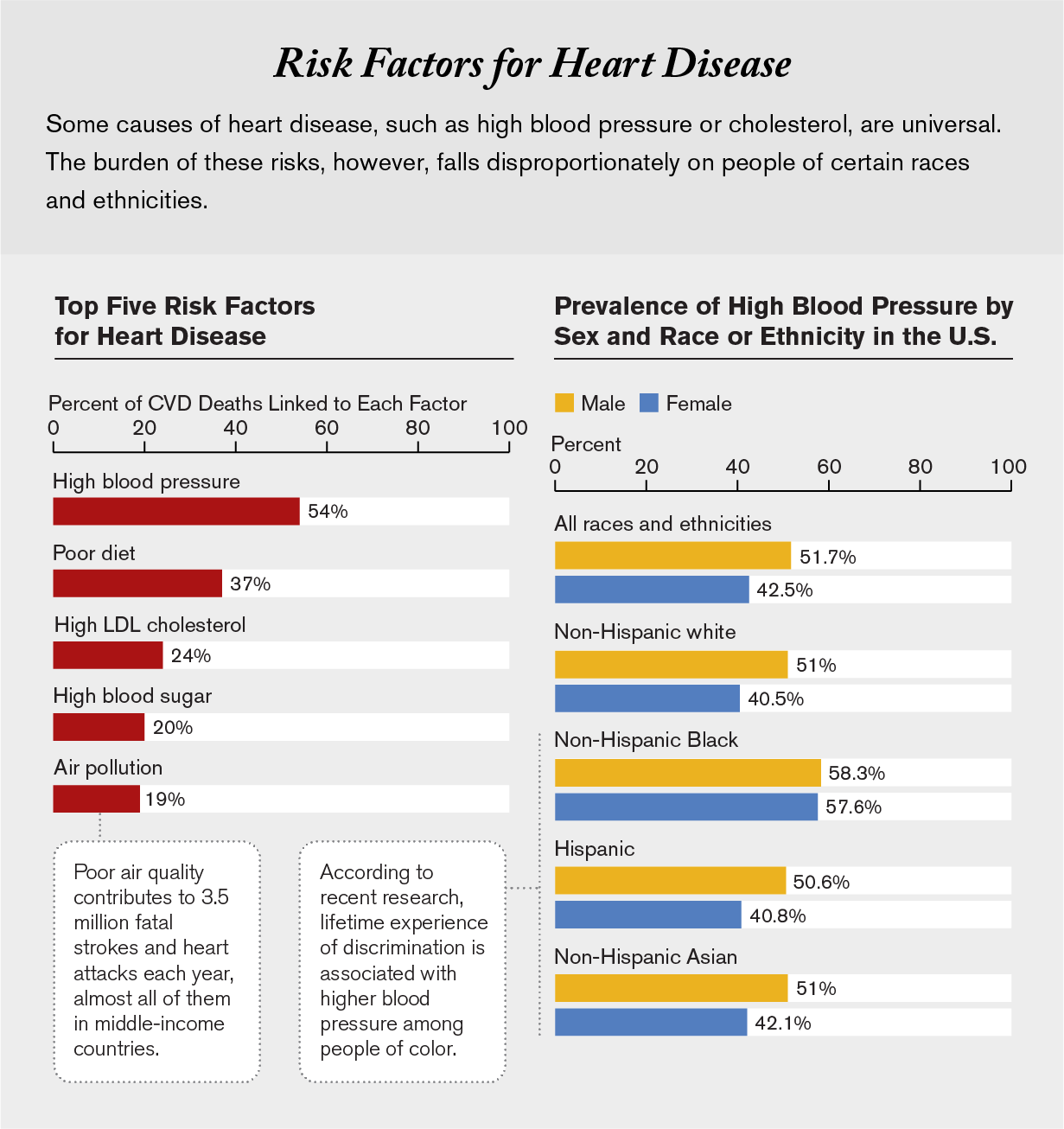
World wide, folks of low socioeconomic standing or those that stay in meals deserts are the most definitely to have diets excessive in sodium and saturated fat and low in contemporary produce. In a examine of 195 international locations revealed within the Lancet, researchers discovered that such diets stay the main reason behind coronary heart illness. Individuals eat this fashion out of necessity, not selection. “The truth is that wherever you might be, the most cost effective solution to eat is usually the least wholesome,” Banerjee says. Internationally, extremely processed meals have grown extra frequent and accessible—extra so than contemporary vegatables and fruits—a minimum of partly attributable to subsidies that usually make junk meals cheaper even within the poorest communities.
In lots of low- and middle-income international locations, charges of weight problems and diabetes initially rose quickest in city areas. Now charges are rising in rural areas as nicely, Patel says. These shifting developments, that are prone to lead to extra situations of coronary heart illness, imply the situation has moved firmly past being a illness of affluence or sedentary life related to metropolis dwelling.
Over the previous twenty years Patel’s work has centered on tribal communities in rural India. She spent just a few years within the village of Juna Mozda, within the western Indian state of Gujarat, and now focuses on understanding coronary heart illness danger components amongst its residents. Most of Juna Mozda’s residents are Adivasis, members of tribal communities. “Among the highest charges of hypertension are amongst these Indigenous communities, who are sometimes the poorest,” Patel says.
Ishwar Vasava, a farmer and social activist who has lived in Juna Mozda all his life, says he has observed a shift in folks’s diets through the years: extra sugar spooned into tea, conventional grains changed with rice, and desserts and fried treats now part of each day routines. Alcohol use is a priority, too, Vasava says, particularly in younger males who return to the village after years of working in adjoining industrial cities. “I do not see a lot of a distinction between our life within the village and that of town anymore,” he says.
City or rural, merely telling folks to eat higher and drink much less alcohol is unlikely to handle rising charges of heart problems. “We inform the story that folks can change their danger themselves,” says Joel Kaufman, an epidemiologist on the College of Washington. “However folks cannot change their eating regimen and life-style as a lot as we might wish to assume.”

Biased Advantages
In high-income international locations, lifestyle-based modifications have clearly helped lower charges of coronary heart illness: Smoking bans, consciousness campaigns and different insurance policies limiting tobacco use have made giant contributions to the lower in deaths from heart problems. So have advances resembling higher screening checks and prescribed drugs. Drugs for treating diabetes, hypertension, excessive ldl cholesterol, and different circumstances have proved so efficient that they’re now on the World Well being Group’s listing of important medicines for all international locations.
The blood checks most frequently used to prescribe these medication sadly don’t work equally nicely for everybody, as a result of they had been developed utilizing knowledge from males of European ancestry. The hemoglobin A1C check for diabetes (which, untreated, is a danger issue for coronary heart assaults) doesn’t work for people who find themselves of Asian or African descent if they’re anemic or aren’t obese. And probably the most generally used ldl cholesterol and triglyceride assessments don’t work as nicely to evaluate danger amongst Black people within the U.S. Even when check outcomes present regular ranges of triglycerides, statistics from the Facilities for Illness Management and Prevention present that Black folks expertise greater charges of hypertension than white, Hispanic or Asian teams, says Anne Sumner, an endocrinology researcher on the Nationwide Institute of Diabetes and Digestive and Kidney Ailments. “Well being disparities aren’t simply associated to not getting access to care. It’s important to have entry to the precise screening instruments, too.”
Exactly how a lot hurt is brought on by inaccurate screening instruments is hard to know for sure. Shortly after her coronary heart assault, Carter-Williams regarded by means of her previous medical information and located some numbers highlighted as irregular. When she requested her medical doctors concerning the outcomes, she says, “they actually couldn’t give me a proof apart from ‘it isn’t excessive sufficient for us to be involved.’” She solely started to obtain ldl cholesterol medicine 10 months later, after her stroke.
Even when check outcomes are correct, limitations to remedy persist, notably in low- and middle-income international locations. It could possibly show almost not possible for some folks—just like the farmer who spends his days doing guide labor—to get to a clinic within the first place. In South Africa, backed well being care ensures that sufferers at many clinics don’t pay for preventive medication, says Kengne of the South African Medical Analysis Council. “If they will get to the clinic, the medicine is free,” he says. “However the transportation value to get there” is the issue.
The price of drugs in addition to their availability hinders entry to medication in lots of low- and middle-income international locations. In a 2020 examine of 21 international locations revealed in BMJ International Well being, researchers linked the inaccessibility of vital medicines to greater odds of incapacity and demise from coronary heart illness. Medication that deal with diabetes or hypertension can be found to solely about 50 to 60 % of the inhabitants in each high-income international locations and low- and middle-income international locations. Within the latter case, a month’s value of brand-name medicine usually prices six days’ wages, whereas generics value about two days’ value. “The most typical purpose folks give me for stopping their medicines is monetary,” says Jaideep Menon, a heart specialist on the Amrita Institute of Medical Sciences and Analysis Middle in Kochi, India. “One other is as a result of the medication aren’t accessible in a pharmacy close to them.”
Gender, age, caste and socioeconomic standing all decide who will get care, Menon says. Discrimination primarily based on these components leads to what researchers name “social deprivation”: restrictions in an individual’s capacity to entry well being care.
These biases aren’t restricted to low-income international locations. They steadily stop entry to high quality care in high-income international locations, too, notably if somebody is Black or feminine. “The locations the place we begin to see a gender divide and elevated coronary heart illness charges in ladies” is in locations the place they expertise discrimination, says Mount Sinai heart specialist Mehran. “That features proper right here within the U.S., the place there’s discrimination towards them primarily based on earnings, schooling, and different components.”
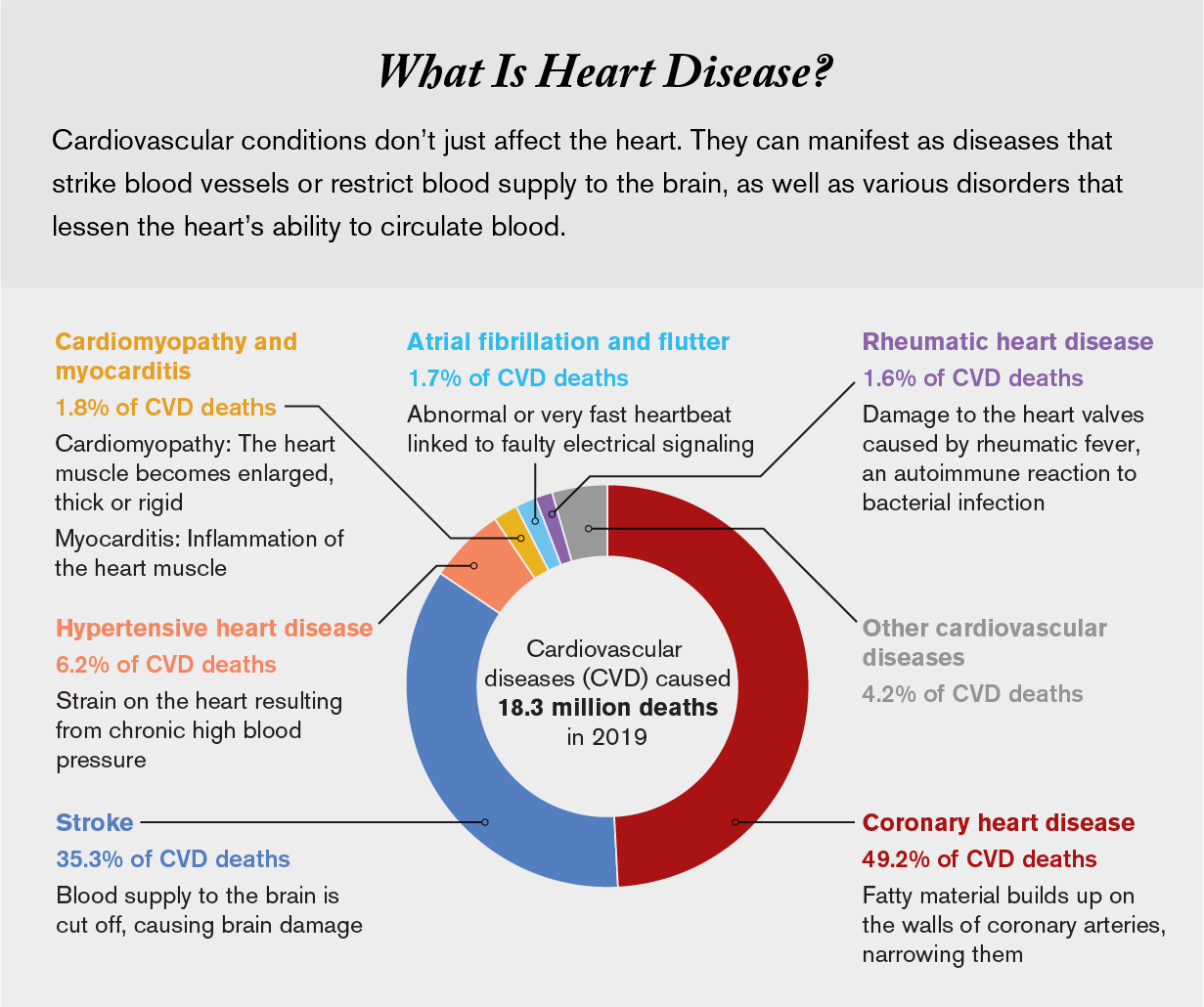
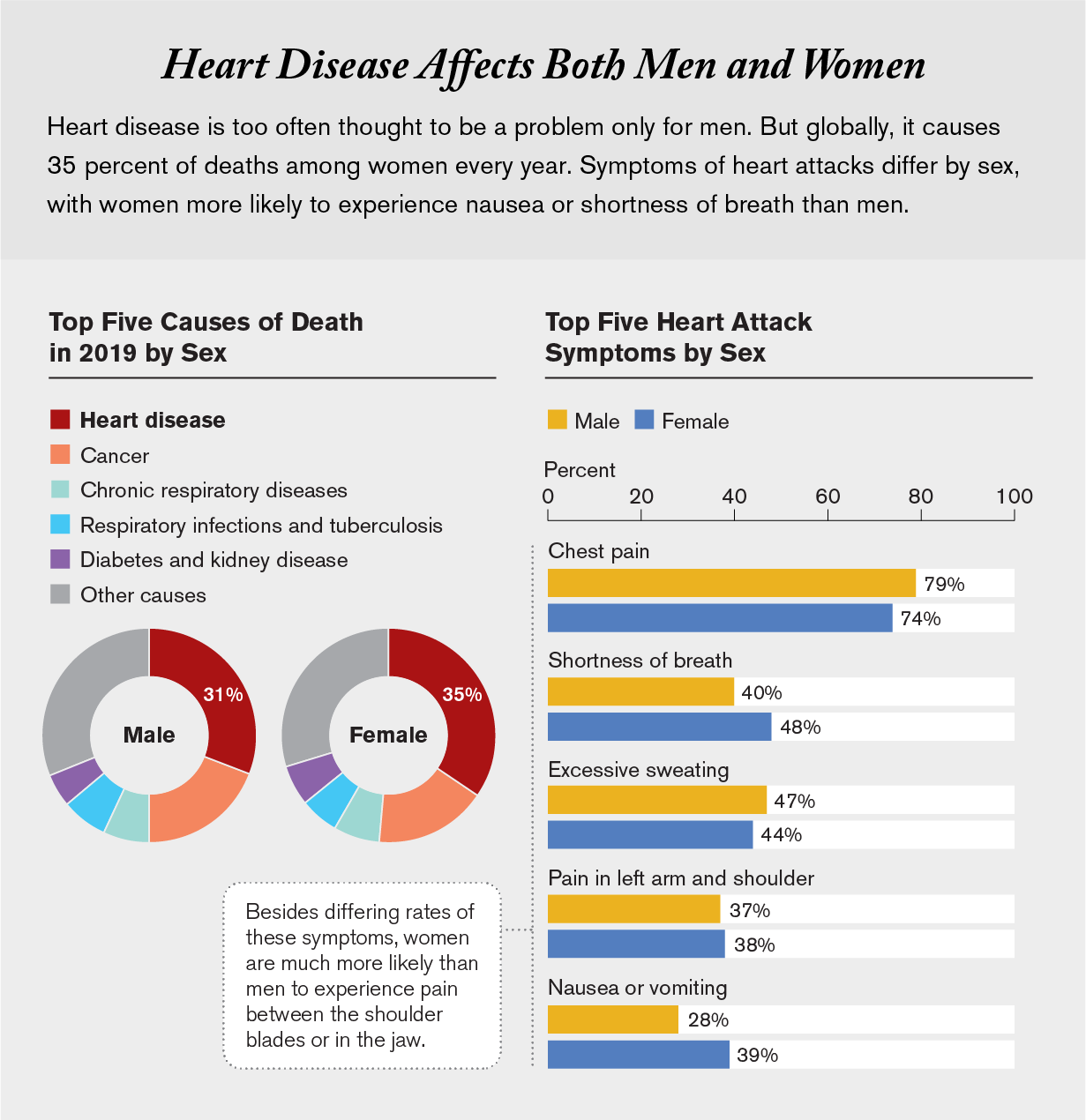
Ladies in cardiac misery are much less prone to be observed or given well timed care. Coronary heart illness and stroke trigger 35 % of deaths in ladies, however their signs are totally different from males’s, and surveys present that physicians are much less assured diagnosing coronary heart assaults in ladies than they’re in males. They’re extra prone to attribute a lady’s coronary heart assault signs to abdomen upset or psychological well being points. And ladies—notably younger Black ladies—are much less prone to obtain remedy, both preventive or as soon as a coronary heart assault has already occurred.
For her half, even after she had been identified with cardiovascular points, Carter-Williams was advised nothing was improper and to “cease stressing out over her job,” she says. She was by no means examined for blocked blood vessels, one thing that will increase somebody’s odds of one other coronary heart assault. Regardless of a household historical past of coronary heart illness and earlier blood checks exhibiting excessive levels of cholesterol and elevated blood stress, she acquired no prescription drugs.
9 months after her first hospital keep, Carter-Williams collapsed at work, unable to stroll or keep in mind her title. This time the hospital doctor suspected seizures. Carter-Williams and her husband weren’t satisfied. After she was discharged, the couple discovered a brand new neurologist, a Black lady, who identified her as having had a stroke.
The stroke left Carter-Williams unable to stroll or sustain along with her job. She took early retirement on the age of 42. And though she is on the mend, she has additionally taken steps to scale back her odds of experiencing discrimination. After eight years of missed diagnoses, she says, “I fired each one in all my medical doctors who did not appear to be me.” Her new care crew are both Black or members of different minority teams, she says. “I needed individuals who may perceive that there’s bias.”
Floor Realities
Inequity endures as a result of it’s rooted in so many sources: unconscious and aware bias, centuries of racism marginalizing folks of colour, a historical past of forcing these of least means and energy into environments which might be probably the most polluted.
That legacy stays a actuality for folks of colour or low socioeconomic standing world wide. Analysis on social determinants of well being lags behind progress in drug growth for diabetes and hypertension. Beginning in 1988, 40 years after the Framingham examine started, researchers launched three comparable efforts to grasp excessive charges of coronary heart illness in Black, Hispanic and Native American communities. Over time these and different research have begun to disclose the significance of discrimination as a danger issue for illness. One examine in 2017 in JAMA Inner Drugs discovered that Black individuals who lived in additional segregated neighborhoods skilled better charges of hypertension. After they moved to much less segregated communities, their blood stress improved.
“Segregation is an efficient proxy for lots of the issues we consider after we consider structural racism, together with schooling, incomes potential and wealth,” says Kiarri Kershaw, the social epidemiologist at Northwestern College who led the work. The brunt of discrimination is borne out in different analysis, too. Research in Brazil, the U.S. and different international locations have proven that individuals who expertise on a regular basis discrimination, resembling being handed over for a promotion or being harassed by neighbors, are likely to have greater charges of hypertension. These social experiences are layered over long-standing laws and insurance policies that exacerbate inequity. Discriminatory practices in housing and the event of freeways, mines or factories normally lead to low-income neighborhoods or marginalized communities bearing the influence of each air and water air pollution.
Meals coverage is equally biased. Governments in lots of international locations impose decrease taxes on the sale of extremely processed meals resembling refined sugar or oils. Recipients of presidency subsidies—who’re normally poorer—usually tend to eat such merchandise. They’re additionally much less possible to have the ability to afford medicines for persistent circumstances resembling hypertension or diabetes that end result from extra consumption of those meals. Funding to enhance medical take care of these precursors to coronary heart illness has did not sustain with the surge in circumstances, partly as a result of the burden of infectious ailments has but to wane.
Altering the social and political programs that exacerbate coronary heart illness is a fancy, unwieldy course of. International insurance policies proceed to prioritize financial growth over the well being of probably the most weak communities on the earth. Which suggests, Menon says, “marginalized teams are likely to lose out on all fronts.”
This text is a part of “Innovations In: Health Equity,” an editorially unbiased particular report that was produced with monetary help from Takeda Pharmaceuticals.








{kind=link}